About Cancer Surgery
Understanding Cancer Surgery: Guide for Patients and Families
Surgery is the oldest form of cancer treatment. It also plays a key role in diagnosing cancer and finding out how far it has spread (a process is called staging). Advances in surgical techniques have allowed surgeons to operate on a growing number of patients and have good outcomes.
When a surgeon has to cut into the body to operate, it’s called invasive surgery. Today, operations that involve less cutting and damage to nearby organs and tissues (less invasive surgery) often can be done to remove tumors while saving as much normal tissue and function as possible.
Surgery offers the greatest chance for cure for many types of cancer, especially those that have not spread to other parts of the body. Most people with cancer will have some type of surgery.
How is surgery used for cancer?
Surgery can be done for many reasons. Some types of surgery are very minor and may be called procedures, while others are much bigger operations. The more common types of cancer surgeries are listed here.
Robotic Surgery
Robotic surgery, or robot-assisted surgery, allows doctors to perform many types of complex procedures with more precision, flexibility and control than is possible with conventional techniques. Robotic surgery is usually associated with minimally invasive surgery procedures performed through tiny incisions.
The most widely used clinical robotic surgical system includes a camera arm and mechanical arms with surgical instruments attached to them. The surgeon controls the arms while seated at a computer console near the operating table. The console gives the surgeon a high-definition, magnified, 3-D view of the surgical site. The surgeon leads other team members who assist during the operation.
Often, robotic surgery makes minimally invasive surgery possible. The benefits of minimally invasive surgery include:
- Fewer complications, such as surgical site infection
- Less pain and blood loss
- Quicker recovery
- Smaller, less noticeable scars
Preventive (prophylactic) surgery
Preventive surgery is done to remove body tissue that is likely to become cancer, even though there are no signs of cancer at the time of the surgery. For example, pre-cancerous polyps may be removed from the colon.
Sometimes preventive surgery is used to remove an entire organ when a person has an inherited condition that puts them at a much higher risk for having cancer some day. For example, some women with a strong family history of breast cancer are found to have a change (mutation) in the DNA of a breast cancer gene (BRCA1 or BRCA2). Because their risk of getting breast cancer is high, these women may want to consider prophylactic mastectomy. This means the breasts are removed before cancer is found.
Diagnostic surgery
This type of surgery is used to take out a piece of tissue (biopsy) to find out if cancer is present or what type of cancer it is. The diagnosis of cancer is made by looking at the cells under a microscope. There are many ways to get a sample of cells from an area that looks like it may be cancer. These are described in more detail in the section called “Surgery to diagnose and stage cancer.”
Staging surgery
Staging surgery is done to find out how much cancer there is and how far it has spread. The physical exam and the results of lab and imaging tests are used to figure out the clinical stage of the cancer. But the surgical stage (also called the pathologic stage) is usually a more exact measure of how far the cancer has spread. To learn more about this, please see our information on Staging. Examples of surgical procedures commonly used to stage cancers, like laparotomy and laparoscopy, are described in the section, “Surgery to diagnose and stage cancer.”
Curative surgery
Curative surgery is done when cancer is found in only one area, and it’s likely that all of the cancer can be removed. In this case, curative surgery can be the main treatment. It may be used alone or along with chemotherapy or radiation therapy, which can be given before or after the operation. Sometimes radiation therapy is actually used during an operation. (This is called intraoperative radiation therapy.)
Debulking (cytoreductive) surgery
Debulking surgery is done to remove some, but not all, of the cancer. It is done when removing all of the cancerous tumor would cause too much damage to an organ or nearby tissues. In these cases, the doctor may take out as much of the tumor as possible and then try to treat what’s left with radiation or chemotherapy. Debulking surgery is commonly used for advanced cancer of the ovary and some lymphomas.
Palliative surgery
This type of surgery is used to treat problems caused by advanced cancer. It is not done to cure the cancer. Palliative surgery can also be used to correct a problem that’s causing discomfort or disability. For example, some cancers in the belly (abdomen) may grow large enough to block off (obstruct) the intestine. If this happens, surgery can be used to remove the blockage. Palliative surgery may also be used to treat pain when the pain is hard to control by other means.
Supportive surgery
Supportive surgery is done to help with other types of treatment. For example, a vascular access device such as a Port-A-Cath® or Infusaport® can be surgically placed into a large vein. The port can then be used to give treatments and draw blood, instead of putting needles in the arms.
Restorative (reconstructive) surgery
This type of surgery is used to improve the way a person looks after major cancer surgery, or to restore the function of an organ or body part after surgery. Examples include breast reconstruction after mastectomy or the use of tissue flaps, bone grafts, or prosthetic (metal or plastic) materials after surgery for head and neck cancers. For more information on these types of reconstructive surgeries, you can read Breast Reconstruction After Mastectomy and Oral Cavity and Oropharyngeal Cancer.
Surgery to diagnose and stage cancer
A biopsy is a procedure done to remove tissue (called a sample) from an area that may be cancer. A doctor looks at the sample under a microscope to see if there are cancer cells in it. Some biopsies may need to be done during surgery. But many types of biopsies are done by removing small pieces of tumor through a thin needle or through a flexible lighted tube called an endoscope. Biopsies are often done by surgeons, but they can be done by other doctors, too. Some of the more common ways to do a biopsy are described here.
Fine needle aspiration biopsy
Fine needle aspiration (FNA) uses a very thin needle attached to a syringe to pull out small bits of tissue. If the tumor can’t be felt near the surface of the body, the needle can be guided into the tumor by looking at it using an imaging test, like an ultrasound or CT scan. The main advantage of FNA is that there is no need to cut through the skin, so there is no surgical incision (in-sih-zhun). A drawback is that in some cases the needle can’t take out enough tissue for an exact diagnosis. A more invasive type of biopsy (one that involves larger needles or a cut in the skin) may then be needed.
Core needle biopsy
This type of biopsy uses a larger needle to take out a core of tissue. A core biopsy sample can be removed with a needle if the tumor can be felt at the surface. Core biopsies can also be guided by imaging tests if the tumor is too deep to be felt. The advantage of core biopsy is that it usually collects enough tissue to find out whether the tumor is cancer.
Excisional or incisional biopsy
For these biopsies a surgeon cuts through the skin to remove the entire tumor (excisional biopsy) or a small part of the tumor (incisional biopsy). They can often be done with local or regional anesthesia. This means numbing drugs are used just in the area where the biopsy will be done. If the tumor is inside the chest or belly (abdomen), drugs that put you into a deep sleep and keep you from feeling pain (general anesthesia) may be needed.
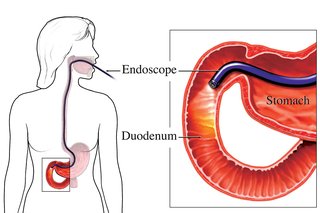
Endoscopy
This procedure uses a long, thin, flexible tube with a viewing lens or a video camera and a fiber optic light on the end. If a video camera is used, it’s connected to a TV screen. This allows the doctor to clearly see any tumors in the area. Endoscopes (end-uh-scopes) can be passed through natural body openings to look at areas of concern in places such as those listed below. Any of these procedures can be called an endoscopy (end-ah-skuh pee), but the more specific name is given as well:
- Pharynx (throat) – pharyngoscopy
- Larynx (voice box) – laryngoscopy
- Esophagus (swallowing tube) – esophagoscopy
- Stomach – gastroscopy
- Small intestine – duodenoscopy
- Colon (large intestine) – colonoscopy
- Sigmoid colon – sigmoidoscopy
- Bladder – cystoscopy
- Respiratory tract (windpipe, smaller breathing tubes, and lungs) – bronchoscopy
Some of the advantages of endoscopy are:
The doctor can look right at the tumor and get a good idea of where it is and how big it is.
A sample of tissue can be taken through the scope to find out if the tumor is cancer.
An open surgical cut (incision) and drugs to put you in a deep sleep (general anesthesia) are usually not needed.